


TRANSFORMing the Primary Prevention of Coronary Heart Disease with AI/CCTA
Will a Cleerly guided paradigm which incorporates newer treatments replace our current ineffective approach and become the key to eliminating heart attack, stroke and other manifestations of ASCVD

In a previous post, the skeptical cardiologist enthusiastically proclaimed CCTA as the ideal tool for assessing stable individuals for the presence, characteristics, and severity of atherosclerotic plaque (aka the atherosclerotic burden) in the coronary arteries.
That CCTA-derived coronary artery disease (CAD) burden is the best clinical tool we have for determining the short and long-term risk of heart attack and stroke, the major manifestations of atherosclerotic cardiovascular disease (ASCVD).
I mentioned that I have been using a process that utilizes AI to streamline the vast amount of information on coronary atherosclerotic plaque present on the clinical CCTA (Cleerly) and have been very excited about that information and how it can be utilized to better risk stratify and measure treatment efficacy.
In this post, I’ll lay out the details of a study being performed utilizing CCTA with Cleerly which has the potential to change (some might say transform) how we detect and prevent ASCVD.
The current standard of care in primary prevention is to plug patient ASCVD risk factors into a formula to estimate risk and use that estimated 10-year risk to guide therapy, an approach which leaves many individuals under-treated and many over-treated.
I've long advocated utilizing coronary artery calcium scans to help us refine individual risk estimation but the future of risk estimation lies with the improved estimate of CAD risk that CCTA represents.
TRANSFORM Details
Per the trial description,
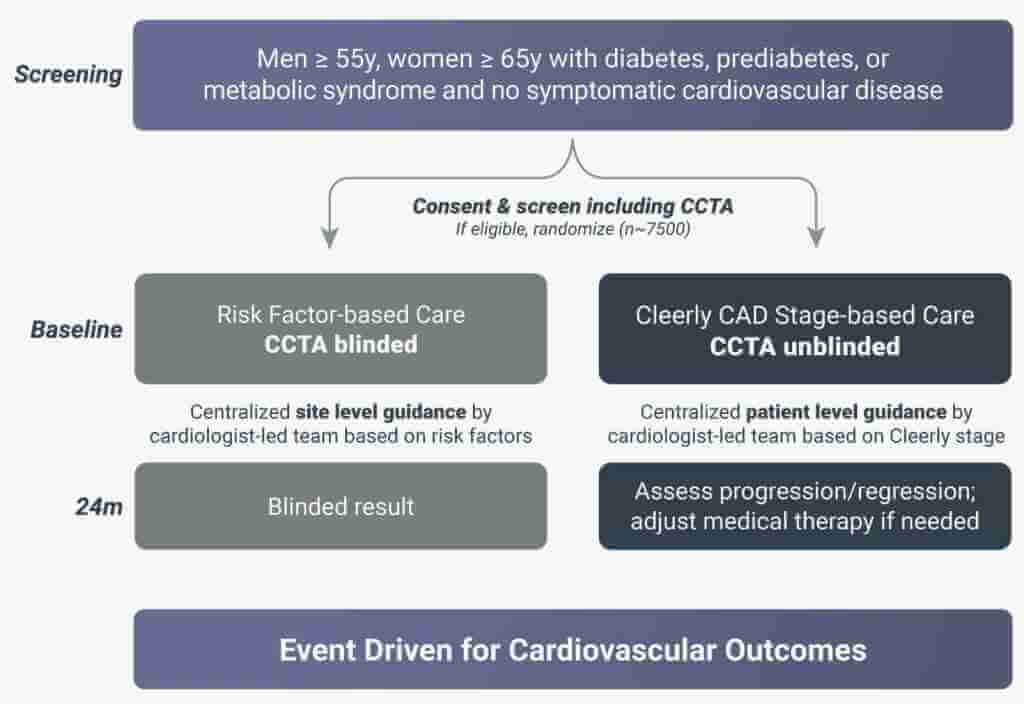
TRANSFORM is a prospective, randomized, open blinded endpoint (PROBE), event-driven, pragmatic trial in patients who are at increased risk for atherosclerotic cardiovascular (CV) disease but with no known symptomatic CV disease. The trial tests the hypothesis that a Cleerly Coronary Artery Disease (CAD) Staging System-based care strategy reduces CV events compared with risk factor-based care
The study chair (highly regarded and seemingly ubiquitous Deepak L. Bhatt, MD, MPH, MBA) gives the rationale as follows:
“Currently, there is no effective way to determine if someone who is healthy but at risk because of diabetes or metabolic syndrome, for example, could experience a major cardiovascular event. TRANSFORM is designed to perform early diagnosis and risk assessment for the severity of plaque using an AI algorithm, then titrate advanced medical therapy to prevent disease progression in those individuals found to be at greatest risk in an effort to reduce heart attack events.”
Organizers like to draw an analogy to the oncology world where "cancers are staged on a scale of I to IV, depending on how much the tumors have grown and spread"
The trial will utilize a four-tier CAD staging system based on a comprehensive assessment of the morphology and composition of coronary atherosclerotic plaque—representing low, mild, moderate, and high risk for future adverse events—and tailor medical therapy based on CAD stage.
“We are hopeful this study will truly be transformative for the practice of cardiovascular medicine,” Dr. Bhatt says. “What we find may allow for a much more refined estimate of patient risk, based on the enormous power of AI in combination with coronary CT angiography, to see if we can measurably improve patient outcomes.”
You can find this graphic at the trial website (www.transformtrial.org) but little other useful information
The trial (A Randomized Comparison of Stage-Based Care Versus Risk Factor-Based Care for Prevention of Cardiovascular Events (TRANSFORM)) is registered at clinicaltrials.gov where you can find more information, including the complete inclusion and exclusion criteria, the primary and secondary endpoints, and to determine if there is an enrolling site near you.
Of the 34 sites listed 9 are in the Los Angeles area

Sadly, Misouri residents have no nearby sites
TRANSFORM Intervention
I couldn't find details of the intervention to be utilized at clinicaltrials.gov other than this brief paragraph:
The Cleerly Stage-Based Care group will receive personalized care centrally managed by a remote cardiologist-led team. They will also receive an initial pre-randomization assessment of current treatment by a centralized cardiology team to optimize care relative to primary prevention guidelines. Cleerly CAD Staging System results will be discussed with participants and serve as the basis for standardized algorithm-supported pharmacotherapy & education, which will be intensified if plaque burden has progressed at 24 months.
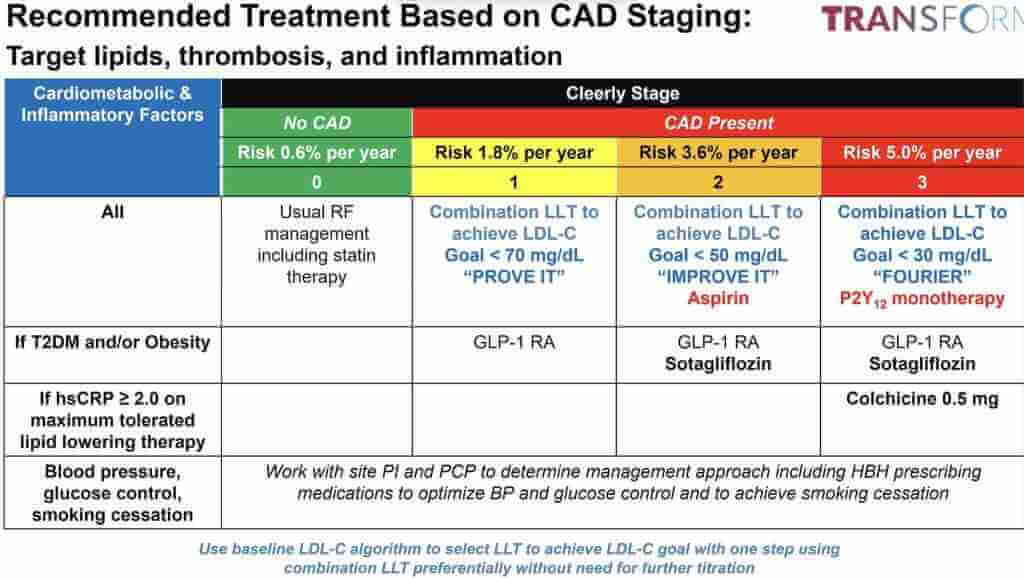
The slide below was presented by Dr. Bhatt at a (Cleerly-sponsored) webinar presenting TRANSFORM. It provides some details on the LDL-C goals and therapies utilized depending on "Cleerly stage" from zero to 3.
A Plethora of Treatments
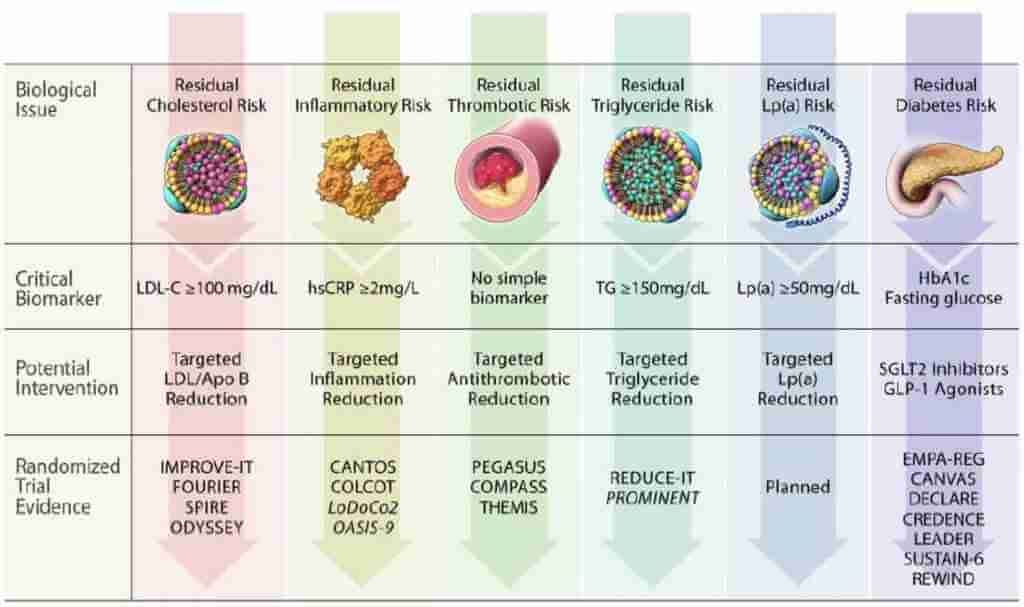
Another slide Dr. Bhatt presented from that (Cleerly-sponsored) Webinar emphasized all the CAD-prevention treatments we now have:
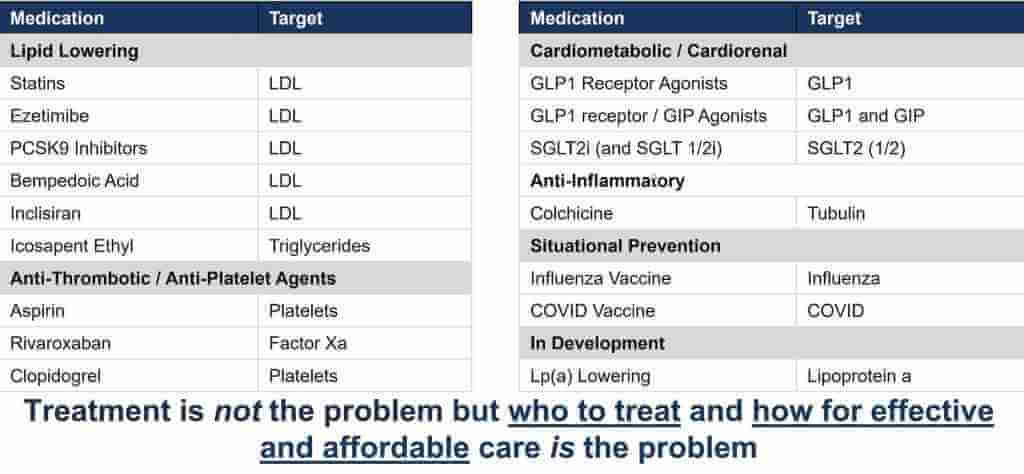
These medications address residual risk biology and are based on multiple recent trials depicted in this very cool Cleerly webinar slide from Dr. Bhatt
Who Should Get the TRANSFORM Approach?
Yes, indeed, we have a plethora of effective interventions and in 5 years we will have a lot more information on how to apply them across the spectrum of CAD risk in primary prevention of ASCVD.
Meanwhile, I offer this TRANSFORMative type of approach to all my patients who have a desire to be very aggressive in reducing their risk of developing ASCVD complications. This includes those interested in primordial prevention (a la Peter Attia), those who have had cardiac events (secondary prevention), and those who have advanced subclinical ASCVD (which is called primary prevention but carries risk equivalent to secondary prevention.)
Many of my patients who are "data-driven" and who want to be very pro-active ask me how we know our treatment of their CAD and ASCVD is effective. They ask if a periodic stress test should be performed (answer is NO!). Prior to CCTA/Cleerly my answer would be that we have no good way of assessing the status of their CAD.
Since realizing the accuracy and quantification inherent in CCTA/Cleerly I have been discussing with patients this type of imaging repeated at 2 year intervals as in the TRANSFORM protocol to "track the plaque" and make therapeutic adjustments as needed based on progression or regression of soft plaque and total plaque burden.
In a subsequent post, I will take a deeper dive into the data supporting my approach.
Clarifyingly Yours,
-ACP
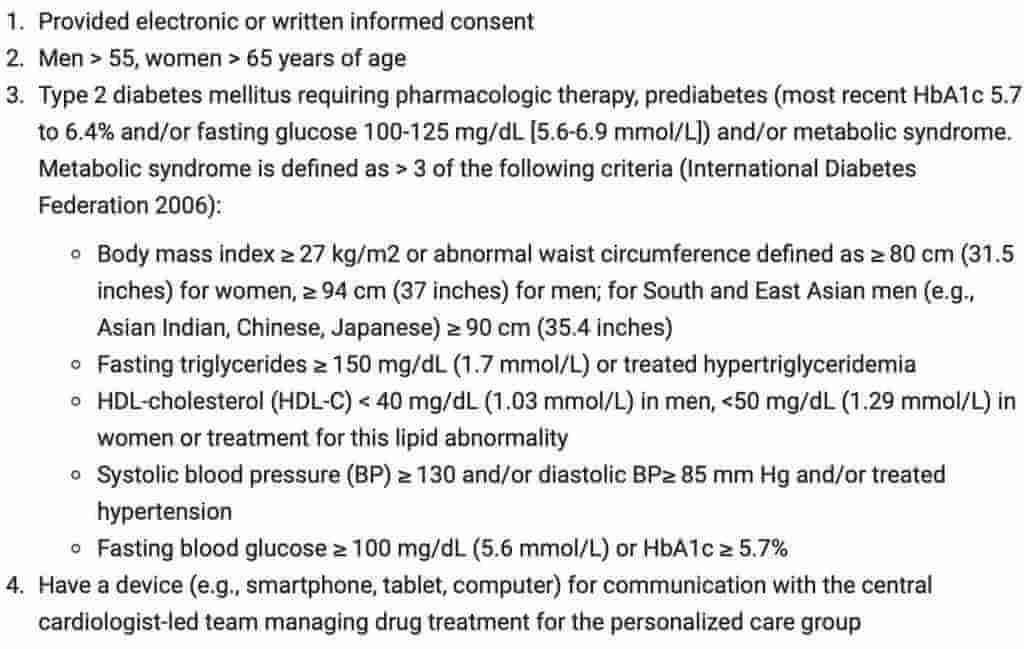
N.B. If you meet these TRANSFORM inclusion criteria to be a participant in TRANSFORM, consider enrolling in it:
BTW, I have no financial interest in or business association in any way with Cleerly and the CCTA scans I order are done at imaging centers which I have vetted as excellent but with which I have no financial connections.
Primary outcome is composite of CV death, MI, stroke (all good), but also Acute limb ischemia (ok)…..and revasc and urgent HF visits. The last 2 are not great for an open label study….when people will be walking around after being told “you have blockages/hardening”….hence more likely to react to minor symptoms…and thus more likely to present for more urgent care which in the US results in more interventions….the evidence notwithstanding.
My CAC is 2536. I understand CTA isn’t effective for CAC >1000. I believe Cleerly uses CTA data. Can Cleerly work for CAC >1000?