


Should You Be Eating Less Salt?
The universal recommendation to lower sodium intake to <2.3 grams per day may be causing more harm than good

The skeptical cardiologist has long questioned the highly ingrained mainstream dietary mantra that all Americans should monitor and reduce their sodium consumption.
I noted in a 2014 post that large observational studies revealed that too little sodium consumption might be as harmful as the consumption of too much sodium.
The PURE study found a steep slope for the association of blood pressure and sodium in participants with sodium excretion (the best way to measure salt intake) of more than 5 g per day. However, only a modest association was noted in those with sodium excretion of 3 to 5 g per day,
There was no significant association between BP and salt intake among those with sodium excretion of less than 3 g per day.
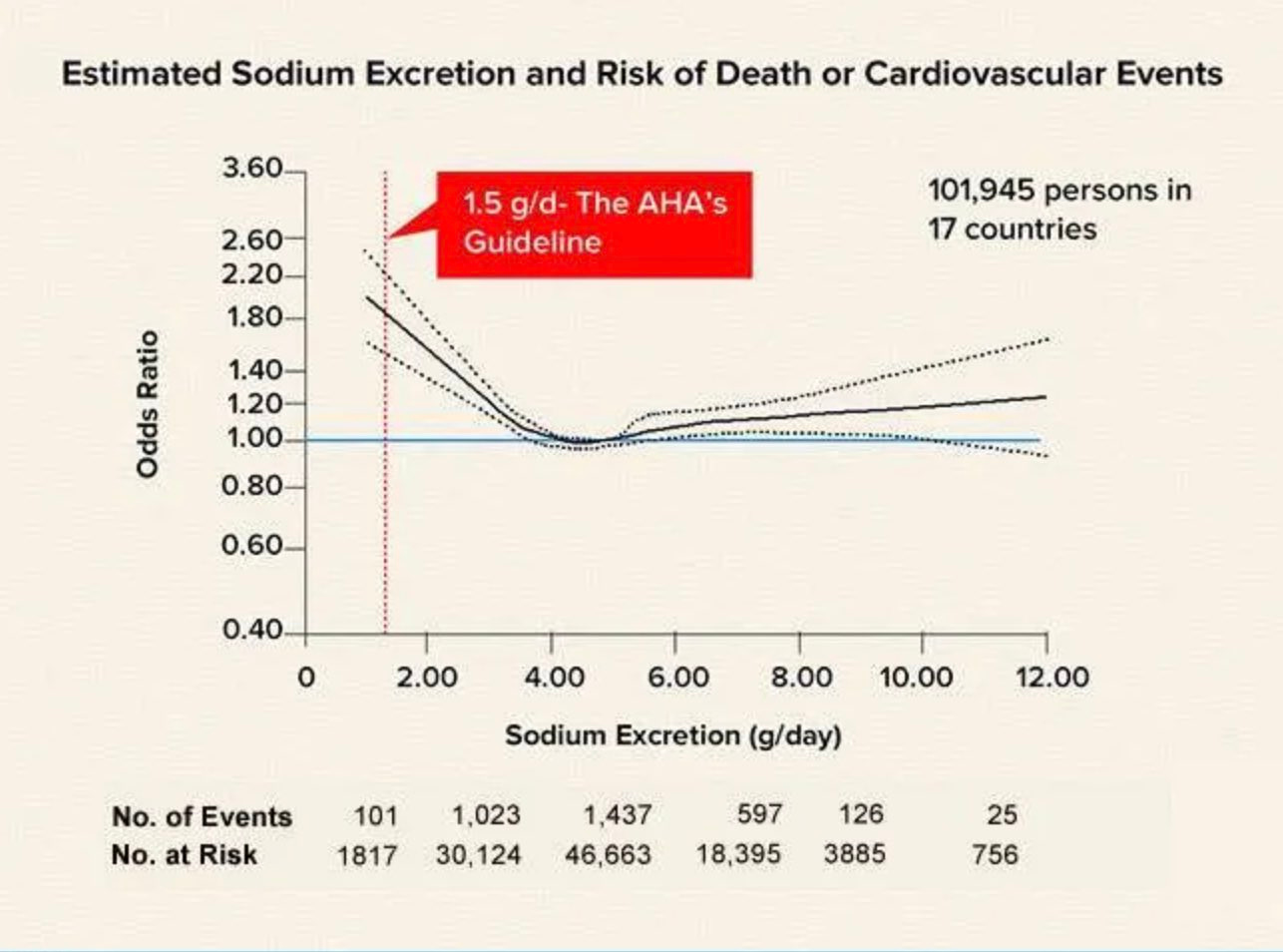
A separate PURE study paper examined the relationship between sodium excretion and death and cardiovascular events
Below is a graph from the PURE study showing that the odds of dying or having a cardiovascular event were double in those with the low sodium consumption of 1.5 grams per day recommended by the American Heart Association and the Dietary Guidelines for Americans.
Americans average 3,400 mg per day of sodium consumption, putting them in the range of 3 to 6 grams per day, which is associated with the lowest risk of cardiovascular death. Lower sodium consumption has minimal effect on BP.
However, the Dietary Guidelines for Americans recommends adults limit sodium intake to less than 2,300 mg per day—that’s equal to about 1 teaspoon of table salt.
These data convinced me that most individuals who are following a Mediterranean diet do not need to be concerned about their salt consumption.
What’s New With Salt Reduction
I was stimulated to review my lax recommendations on sodium after reading about a large randomized trial showing that using a salt substitute significantly lowered stroke risk in a Chinese population (1)
Since my last post on salt, an updated Cochrane analysis of all randomized controlled trials of low versus high sodium was published in 2020.
This analysis looked at 195 intervention studies of 12296 individuals lasting three to 1100 days. Here’s the layperson summary of the findings:
The mean salt intake was reduced from 11.5 g per day to 3.8 g per day. The reduction in SBP/DBP in people with normal blood pressure was 1.1/0 mmHg (about 0.3%) , and in people with hypertension 5.7/2.9 mmHg (about 3%). In contrast, the effect on hormones and lipids were similar in people with normotension and hypertension. Renin increased 55%; aldosterone increased 127%; adrenalin increased 14%; noradrenalin increased 27%; cholesterol increased 2.9%; and triglyceride increased 6.3%.
Clearly, there is no reason to limit sodium consumption to less than 3.4 grams per day if your blood pressure is normal. Furthermore, those adverse hormonal and lipid changes may be why there is a higher risk of dying with sodium intake <3 gms/day.
The Cochrane author’s clinical perspective on their findings:
In white people with elevated BP, sodium reduction decreases BP by about 3.5%, indicating that sodium reduction may be used as a supplementary treatment for hypertension. In Asian and black people the effect of sodium reduction was a little larger than in white people, but at present too few studies have been carried out to conclude differently from that above.
Optimal Sodium Consumption Needs to be Individualized
When I first began attempting to track my own sodium consumption I asked most of the patients I saw in my office about their salt consumption. None of them could tell me what their average daily salt consumption was. However, almost to a man (or woman), they told me they had been consciously limiting their salt consumption because they knew this was healthy.
Thus, the 35-year-old white woman with a blood pressure of 110/50, palpitations, and periodic dizzy spells is following the same recommendations to limit salt consumption as the 70-year-old African-American with poorly controlled hypertension.
In addition, your body’s need for salt varies substantially depending on how active you are and the ambient temperature. Sweating and salt loss vary widely between individuals and over time in the same individuals. Scientists have studied professional tennis players and measured their sweat loss to be as high as 2.5 L/ hour while playing singles in hot circumstances. A liter of sweat contains around 920 mg of sodium thus these tennis players were losing 2.3 grams per hour of sodium!
It is common for my patients to note that during the summer months their blood pressure drops when they spend time gardening or if they have a job that requires heavy exertion in hot conditions. Often a downward adjustment in blood pressure medications is needed to account for this (especially if a diuretic is one of their BP drugs).
These variations in salt loss in the context of large variations in cardiovascular physiology and blood pressure regulation between individuals provide further support for abandoning the ultra-low salt limits suggested by the AHA and the USDA.
Moderation may not be best for all things in diet (ultra-processed foods and added sugar come to mind) but for salt consumption moderation appears best.
My Recommendations on Salt Consumption
Here is what I tell my patients about salt (2):
Spend a day or two accurately tracking your consumption of salt to educate yourself. I found this app to be really helpful.
Recognize that not everybody needs to follow a low-salt diet. If your blood pressure is not elevated and you have no heart failure you don’t need to change your salt consumption.
If your blood pressure is on the low side and especially if you get periodic dizzy spells, often associated with standing quickly liberalize your salt intake, and you will feel better.
If you have high blood pressure, you are the best judge of how salt affects your blood pressure. In the example I gave in a previous post, my patient realized that all the salt he was sprinkling on his tomatoes was the major factor causing his blood pressure to spike.
The kidneys do a great job of balancing sodium intake and sodium excretion if they are working normally. If you have kidney dysfunction you will be more sensitive to the effects of salt consumption on your blood pressure and fluid retention.
If you are following a Mediterranean diet with plenty of fresh fruits and vegetables and minimal processed and packaged food you are going to be in the ideal range for both potassium and sodium consumption.
Public health experts are always seeking a “one size fits all” message to give the public. In the case of salt consumption, however, the message of less is better does not apply to all.
Saltatorily Yours,
-ACP
(1) The Chinese salt substitute study is intriguing. We will delve into this in detail down the line. It does suggest, however, that increasing potassium consumption is more important than lowering sodium consumption
(2) I’ve also written about cooking with salt here. That post from 2016 includes observational data suggesting those with hypertension benefit from lowering salt consumption >7 gms/day down to 4-5 grams/ day and comments on Kosher salt.
Alice,
Is this a good thing or a bad thing?
Dr. P
Carvel,
Could you elaborate in more detail on this?
Dr. P