


Is My Ascending Aorta Truly Enlarged or Enlarging?
Echocardiography is our primary imaging modality for screening most cardiac abnormalities but errors in recording and measurement are common and complicate between study comparisons

The recent sudden, unexpected death of prominent soccer journalist Grant Wahl from a ruptured thoracic ascending aortic aneurysm prompted the skeptical cardiologist to resuscitate his dormant article on measuring the aorta by echocardiography.
If you’ve had an echo performed by a reputable facility, parts of your aorta were imaged and measured. If the reported size of your aorta changes from one echo to another is this cause for concern?
For 50 years the echocardiogram has been the primary tool of cardiologists to evaluate the size of cardiac structures, the function of valves and cardiac muscle, and the pressures in the heart.
More than 30 million of these harmless and painless exams are performed annually in the US and many of them contain inaccurate information.
I discussed in detail how and why you can get bad information from the echo report here. Errors can occur due to technician incompetence or sloppiness in the initial recording and measuring or due to physician incompetence or sloppiness in the interpretation.
Hundreds of measurements can be made on an echocardiogram: what is measured, how measurements are made, and what is reported vary dramatically from one facility to another.
Of all cardiovascular structures, I see the most variation and error occurring in the recording and measurement of the ascending aorta.
What is the Aorta?
Of all the cardiovascular structures, I see the most variation and error occurring in the recording and measurement of the ascending aorta. The ascending aorta is part of the thoracic (chest) aorta. Portions of the aorta below the diaphragm (the abdominal aorta) can be imaged by echocardiography but in general screening for and follow-up of abdominal aneurysms is done using either abdominal ultrasound, CT or MRI imaging.
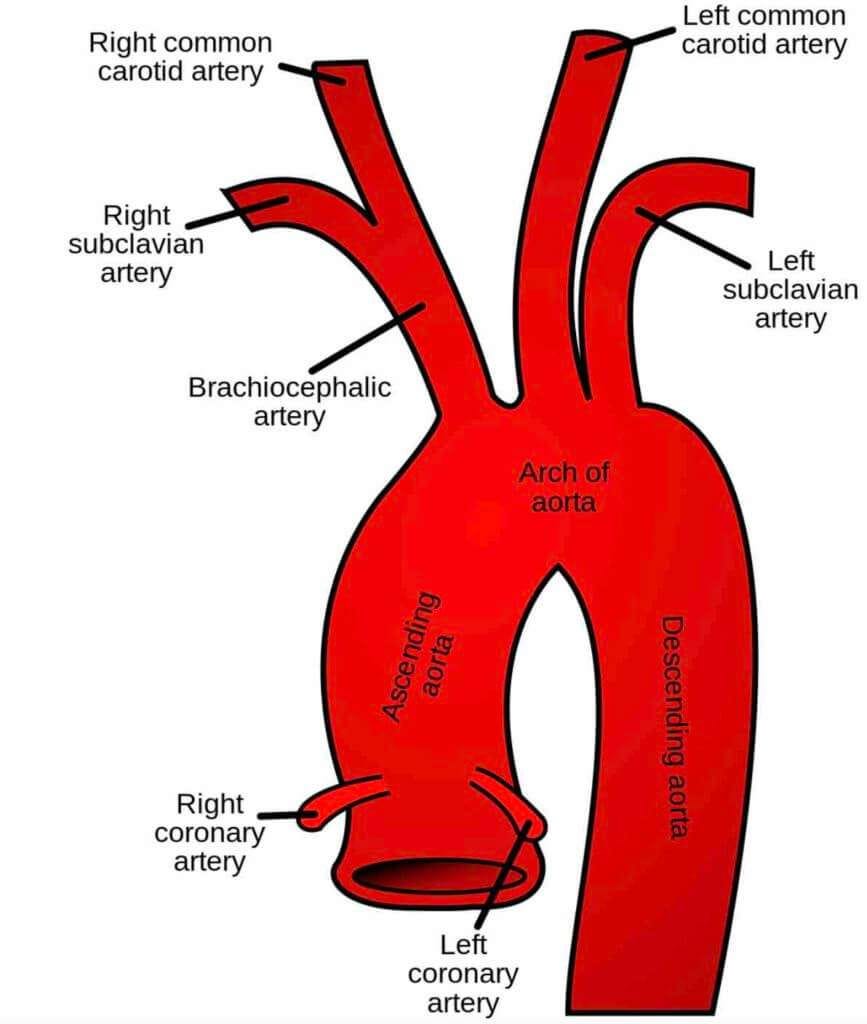
As it is in the chest (aka thorax) it is part of the thoracic aorta After reaching the top of the chest, the aorta reverses direction, heads south, descending toward the feet (assuming an upright stance), and becomes the descending thoracic aorta.
The bend of the thoracic aorta thus created is termed the aortic arch, and gives off the main arteries to the right arm, the brain, and the left arm.
Enlargement of the ascending aorta (Asa) results in an ascending aortic aneurysm. The larger, the aortic aneurysm the higher the likelihood that a tear (dissection) or rupture will occur. A dissection or rupture of the ascending aorta is a life-threatening event requiring emergency surgery thus accurate, precise echo measurement of the AsA is hugely important.
It should be noted that you can have severe enlargement of your AsA and have no symptoms.
What is the Significance of Increasing Size of the Aortic Root or Ascending Aorta?
A reader question triggered me to write on echo evaluation of the aorta:
I am a 37-year old male, about 6'1 and 170 pounds. I just got an echo (at the local hospital) which showed my aortic root dimension (in 2D) as 3.1 cm (which apparently is normal?). However, I previously got an echo in 2008 and my report from back then says my aortic root diameter was 2.1 cm (in M-Mode). Seeing that it grew by 50% (1 entire centimeter in 14 years) was quite alarming. Should I just assume that it was under-measured before? Or might it actually be growing that rapidly? Would 2.1 cm have been unreasonably small back then?
What Was the Indication for the Echocardiogram?
Whenever an echo is done there should be a good reason. If there is no good indication for the study to be performed we run into the problem of false positives-things that are interpreted as pathologic or abnormal when the truth is they are normal and of no consequence.
Hopefully, there was something on your exam or your history that warranted an echocardiogram. Such things would include the findings of a heart murmur, a family history of aortic dissection or aneurysm, or symptoms like shortness of breath or chest pain that suggest a cardiac problem.
I've written in detail about the problems with screening echocardiograms in a post entitled "Shoddy Cardiovascular Screenings Are More Likely to Cause Harm Than Good."
What Part of the Ascending Aorta was Measured?
The reader wrote "I just got an echo (at the local hospital) which showed my aortic root dimension (in 2D) as 3.1 cm (which apparently is normal?)"
The ascending aorta is connected to the left ventricle by the aortic root, depicted below.

Now that we have two-dimensional echocardiography, these measurements should all be measured and reported along with their normal ranges. Ideally, one should see those 3 measurements plus a measurement of the ascending aorta 2 cm further along (distal) from the sinotubular junction. Most enlargement (often called dilatation) of the AsA occurs distal to the sinotubular.
A well-trained, good sonographer will optimize the images for the aortic root structure measurements but then shift both the location of their ultrasound probe and the angle of the probe to optimize the more distal portions of the ascending aorta and measure the largest diameter. Unfortunately, this does not always happen and a poorly-trained, sloppy or lazy sonographer (yes these exist as do poorly-trained, sloppy and lazy cardiologists) may easily miss a large aneurysm.
A measurement of 3.1 cm would be normal for the sinotubular junction or ascending aorta. In a man, the AsA is considered normal up to 3.8 cm and in women up to 3.5 cm (2).
The measurement of 2.1 cm is below the normal range for M-mode measurements of the aorta and likely represents an error due to one of three things; 1) poor sonographer recording 2) poor sonographer measurement 3) typo.
What this reader had reported on the study from 14 years ago we can only guess at unless we were to take the time to get the images burned to a disc and mailed to us (1). This is unlikely as most facilities will not have retained images from echos more than 5 to 10 years. The number 3.1 cm would be normal for sinotubular junction or ascending aorta.
Nonshoddily Yours,
-ACP
N.B. (1) It boggles the mind that in 2022 it is so difficult to get images from cardiac echos previously performed on our patients. It doesn’t matter if the echo was performed in a hospital or a doctor’s office it is like pulling teeth to get the CD burned and mailed or expressed to my office. Then it is an adventure trying to read the images off the CD or have them imported into our imaging storage system. We have the capability of viewing these from a link to the cloud but this is very rarely made available to doctors. The difficulty of this process contributes to repeat, often unnecessary testing.
N.B. (2) As there is a correlation between patient size (BSA) and size of the AsA some centers/authorities recommend reporting the AsA dimension divided by the BSA. However, when looking at cut-offs for consideration of surgery on an AsA aneurysm, the uncorrected AsA is always the one used (e.g. 5.5 cm.)
N.B. (3) The Mayo Clinic has a good article here that provides information on treatment options available for severely enlarged thoracic aortic aneurysms. Although that article mentions an endovascular (meaning without open heart surgery) repair technique please note that this only applies to the less life-threatening descending aorta aneurysm.
Marcus,
Your case touches on two of the issues I mentioned.
First, the aortic root bulges at the sinuses of Valsalva and 4.0 cm would be normal if that was the measurement. On the other hand if this was above the sinuses and truly measuring the ascending aorta it would be enlarged. Echo reports should state very clearly where these measurements are taken and they should be compared to the normal range for the appropriate site.
Second, assuming your 4.0-4.1 cm measurement was the ascending aorta, given your height this may not be of concern. Some studies (https://www.acc.org/latest-in-cardiology/journal-scans/2018/05/11/11/30/height-alone-rather-than-body-surface-area) show that when you index the aortic diameter by height risks are better predicted.
Aortic ectasia is another term for enlargement (dilatation) of the aorta
Most experts and guidelines would advise regular follow up of this finding. In this kind of case if stable over many years I would repeat the echo every 2-3 years.
Dr. P
Thanks for posting this. I am a 66yo white man. in Dec 21 I was told I had a root aneurysm measuring 5.0cm. (I have HBP) In early 2023 I had a CT scan, and the swelling measured 4.9cm. In July 2024 I had another CT scan, and the swelling measured 4.8cm, and the descending part measuring in at 4.1cm (they called it 'ectasia'). It seems my root aneurysm is shrinking! But I'm suspicious of these results, because they may not be measuring it at the same places, with the same degree of care. I wish I didn't have these concerns.