

Coronary CT Angiography: Is it Time to View Your Coronary Arteries Cleerly?
Coronary CT Angiography: Is it Time to View Your Coronary Arteries Cleerly?
The best method for visualizing the plaque in coronary arteries gets better with a boost from artificial intelligence

In 2007, at a time when I was leaving a cardiology practice in Louisville and moving to one in St. Louis, I decided that I needed to add the interpretation of coronary CT angiograms to my cardiac imaging toolkit.
For decades, the so-called “cardiac catheterization” (typically shortened to "Cath") had been the only method for directly visualizing plaque and blockages in the coronary arteries.
A cardiac cath is considered an “invasive” procedure in contrast to the “non-invasive” cardiac imaging tests I had become an expert on like echocardiography and nuclear stress testing.
The first invasive cardiology procedure is generally credited to an English parson, Stephen Hales, who, in 1711 began inserting brass pipes into the carotid artery of horses and other animals.
In 1958, Mason Sones, accidentally injected radiographic contrast material into the origin of the right coronary artery of a patient, thereby performing the first invasive coronary angiogram. The patient went into ventricular fibrillation when this happened but was resuscitated.
The coronary CT angiogram (CCTA) does not require a brass tube or the now utilized small, flexible tube (aka catheter) to be inserted into an artery to visualize radiographic contrast material in the coronary arteries which makes it non-invasive and much less risky.
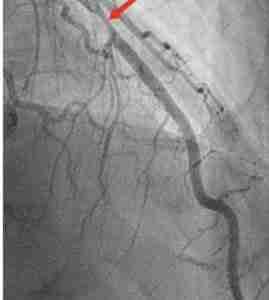
An invasive coronary angiogram (ICA) shows only the lumen of the coronary artery. And it only shows the artery in two dimensions. Patients with advanced subclinical coronary atherosclerosis not uncommonly have "normal" ICAs (see here.)
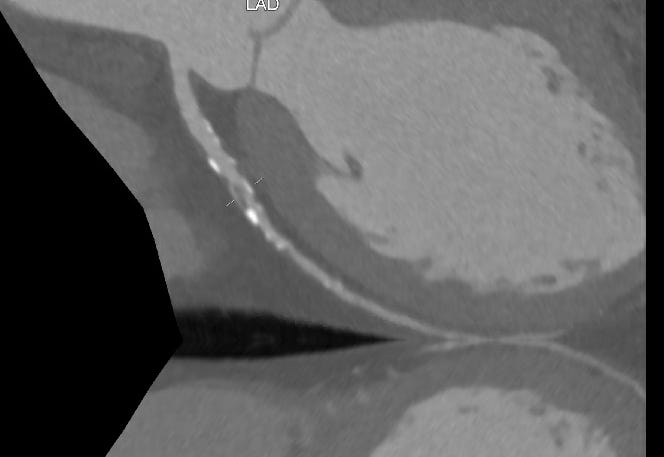
The CCTA, on the other hand, shows both the lumen and the actual atherosclerotic plaque which is within the wall of the artery.
Consequently, the CCTA is a much better tool for assessing stable individuals for the presence, characteristics and severity of atherosclerotic plaque (aka the atherosclerotic burden).
If you are having a myocardial infarction caused by an occlusive plaque you want to have an ICA as soon as possible: the benefits of opening the occluded artery substantially outweigh the risks of the cath-but for the vast majority of patient situations the CCTA is the imaging tool of choice.
Assessment of subclinical atherosclerotic cardiovascular disease (ASCVD)
I am an enthusiastic advocate of using the coronary artery calcium scan (CAC) to detect and quantify subclinical ASCVD (and have written on this extensively.)
The CCTA is also a far better tool than CAC for assessing the phenotypes of atherosclerotic plaque development in the coronary arteries.
There are several key limitations to CAC.
First, CAC can be zero in younger individuals who have substantial coronary plaque burden. Atherosclerosis begins as non calcified or soft plaque which cannot be quantified on the non-contrast CT scan performed for calcium determination. Soft plaque tends to be more unstable, thus more likely to rupture and cause myocardial infarction. Plaque has to mature or undergo healing before it becomes calcified.
Second, CAC increases over time irrespective of what is done to lower the risk of myocardial infarction and stroke. There is no benefit to repeating a nonzero CAC score in my opinion. The CAC cannot be repeated to gain insights into how effective therapy has been.
Third, although non-zero CAC scores allow us to more precisely estimate ASCVD risk and to better see where each patient sits compared to age and gender-matched peers for plaque burden it does not give us any insights into the relative amount of soft versus calcified plaque.
Coronary CT Angiography sees all
The landmark ISCHEMIA trial was instrumental in demonstrating the utility of CCTA in patients with stable ischemic heart disease.
As noted in a recent review on precision prevention based on coronary CTA-derived coronary atherosclerosis:
The characteristics and volume of coronary atherosclerosis are the key phenotypes of CAD and are becoming increasingly important as novel markers for better CVD risk prediction. Given its capability for visualizing the entire coronary arterial tree, coronary CTA allows for quantitative evaluation of plaque characteristics and total plaque volume [reference], and has the advantage of assessing risk using these key CAD data.
Indeed, the information one gains from viewing a high-quality CCTA is remarkable.
While undergoing my training in CCTA in Texas, I had a scan performed on myself. I was 53 years old at the time. I had no symptoms but My father had an MI while playing tennis when he was 60 years old and I had hypertension.
My LDL-C levels weren’t particularly high but I periodically took rosuvastatin after eating particularly unhealthy meals just to be on the safe side (not a recommended protocol.)
The scan showed no calcium in my arteries but did identify a small area of soft plaque in the proximal LAD coronary artery which was in the wall of the artery and not causing any obstruction.
This information could not have been obtained by any other easily available clinical test. An invasive coronary angiogram would have been normal and likely I would have been told I have the arteries of a 20-year-old.
A CAC would have given me a score of zero.
Stress testing whether with nuclear or echo imaging would have been totally normal: I would have passed with flying colors.
Although I knew theoretically it was highly likely I had already built up soft plaque in my coronaries, the direct visualization of the soft plaque in a critical part of my coronary anatomy convinced me to take rosuvastatin daily- something I have done continuously since then.
The CCTA allows complete visualization of the coronary arterial tree and this is a lot of complex, 3-D information. The majority of clinically obtained CCTA reports fail to capture the full breadth of information on atherosclerotic plaque in the coronaries.
True quantitation of the amount, nature, and location of atherosclerotic plaque is not going to be found on clinical CCTA reports. It is far too time-consuming and dependent on the skill, patience, and experience of the individual reader.
As that review on precision CAD prevention notes:
However, such merits are still neglected owing to the lack of a systematic approach to incorporate this information in a clinical setting. Although the evaluation of total coronary atherosclerosis requires time and specialized software, recent technology has made the measurements easier and more suitable for daily use in clinical practice
Enter Cleerly
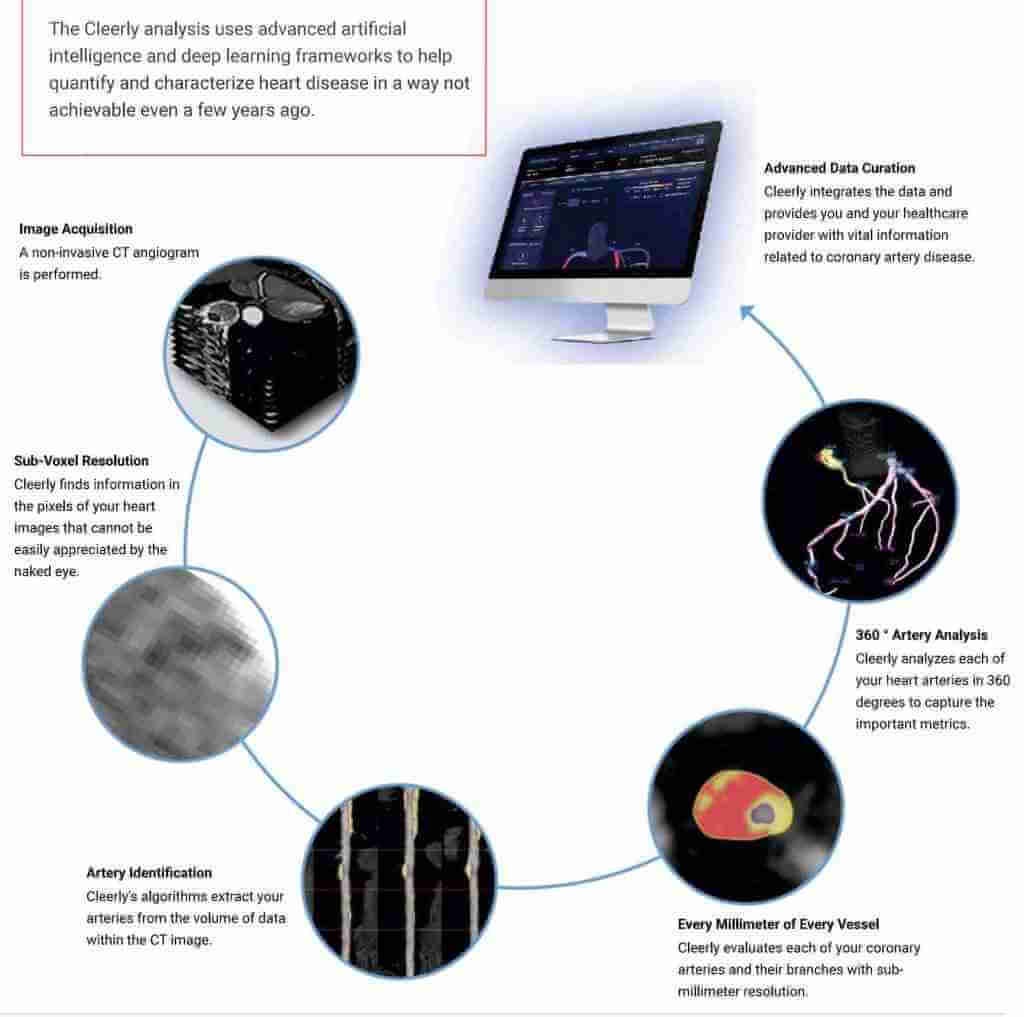
I have been evaluating for the past year a process that utilizes AI to streamline the vast amount of information on coronary atherosclerotic plaque present in CCTA.
Cleerly, the company behind this process describes itself as:
A company on a mission to eliminate heart attacks by creating a new standard of care for heart disease. Through its FDA-cleared solutions driven by artificial intelligence, Cleerly supports comprehensive phenotyping of coronary artery disease, as determined from advanced non-invasive CT imaging. Cleerly’s approach is grounded in science, based on over 10 million images from over 40,000 patients gathered over a 15-year-period in landmark, multi-center clinical trials.
In March of 2024, Cleerly Was granted Breakthrough Device Designation by the FDA for its Coronary Artery Disease (CAD) Staging System.
The CAD Staging System is a noninvasive imaging-based investigational software device that analyzes important and actionable features of coronary atherosclerosis, stenosis and ischemia. Its purpose is to support physicians with a more accurate and personalized risk assessment for patients at risk of major adverse cardiovascular events (MACE), including heart attacks, before they happen.
The Cleerly analysis of a patient's CCTA presents a diagram of each coronary artery with color-coded graphics showing the presence of calcified and soft plaque.
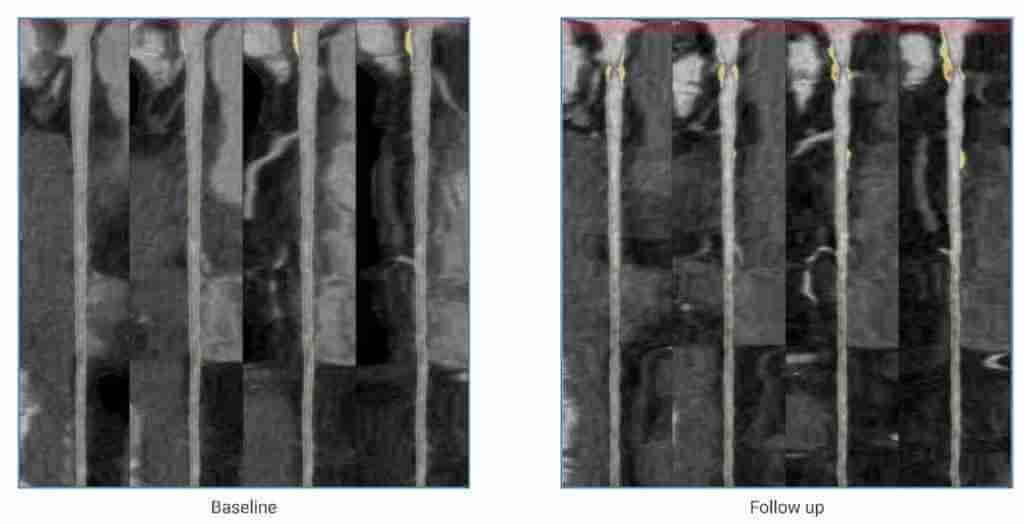
Since I had my first CCTA in 2007 I've been keeping an eye on that soft LAD plaque and subsequent CAC scans have shown the development of calcification.
After experiencing worrisome symptoms I underwent a repeat CCTA with Cleerly AI analysis.
Below is the detailed AI analysis of my LAD coronary. Soft plaque is depicted in yellow and calcified plaque in blue.
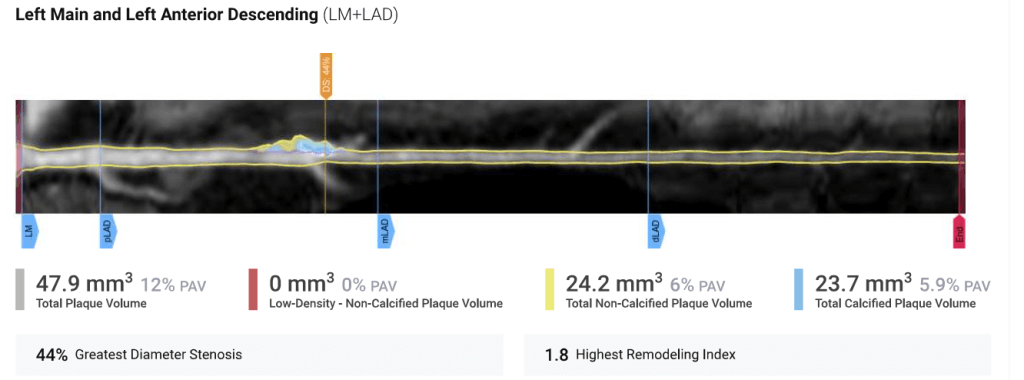
The detailed AI quantification gives precise information on total, non-calcified and calcified plaque volume. That small soft plaque is now larger and 50% of it is calcified plaque.
It also determined that the plaque was causing a 44% diameter stenosis of the LAD, a progression from a subjective <25% stenosis in 2007.
How Should Cleerly Be Utilized: Who Should Undergo CCTA with AI Quantification?
I am very impressed with the information we can get noninvasively on coronary artery plaque in our patients using the Cleerly AI analysis of their CCTAs. It is a big step forward from subjective reader analysis.
We are still learning which patients will benefit from Cleerly and other AI tools applied to CCTA. In Part 2, of this post, I'll discuss the situations where I have been recommending the tool, how the findings can change management, and what scientific studies have shown and hope to show.
Clarifyingly Yours,
-ACP
Thanks for sharing your personal info, even the embarrassing part! :) I look forward to hearing how this has informed your day-to-day lifestyle and medication choices, and whether the knowledge has given you more or less equanimity. I'm also curious to hear your take on the article below. Maybe the improved risk prediction will help doctors more accurately pinpoint who best to target for primary prevention. I do wish the CCT would release the data because their failure to do so leads many folks to reasonably conclude they must be hiding something.
https://www.medpagetoday.com/opinion/second-opinions/110734?xid=nl_secondopinion_2024-06-23&eun=g2093479d0r
Correct me if I am wrong: 'This test is ONLY a predictor for something that can not be stopped, reversed or cured. And while it MAY be useful longitudinally to chart an assumed future demise, the downstream psychological harm to many patients has the POTENTIAL to cause more damage than good or promote any reasonable understanding of the test results.'
Follow up: In what universe would a sane person disclose: "My LDL-C levels weren’t particularly high but I periodically took rosuvastatin after eating particularly unhealthy meals just to be on the safe side (not a recommended protocol.)" ???
(opinion) 6-2-and even you will not answer!