


A Series of Unnecessary Cardiovascular Procedures and Surgeries Culminates in the Death of Philip Roth's Everyman: How You Can Avoid the Same Fate
Earlier this year the skeptical cardiologist wrote about the cardiovascular misadventures of the main character in Philip Roth's novel Everyman.
I had initially intended this as a single blog post but very quickly realized there were more important points about cardiovascular disease management than could be contained in a one-thousand-word post.
After Roth's Everyman is rushed to the hospital to undergo an invasive coronary angiogram he likely didn't need, he is then rushed off to undergo coronary bypass surgery he likely didn't need. In 1998 at the age of 65 he undergoes renal artery stenting for high blood pressure, a procedure now considered of dubious value.
The First Unnecessary Carotid Surgery
One year after his renal artery stent, he had a left carotid endarterectomy (CEA) which he describes as “surgery for another major obstruction, this one in his left carotid artery, one of the two main arteries that stretch from the aorta to the base of the skull and supply blood to the brain, and that if left obstructed could cause a disabling stroke or even sudden death.”
He goes on to describe the procedure in some detail: "the incision was made in the neck, then the artery feeding the brain was clamped shut to stop the blood flowing through it. Then it was slit open and the plaque that was causing the blockage scraped out and removed.”
He is told “from a medical point of view, it was nothing extraordinary, or so he was led to believe by the agreeable surgeon, who assured him that a carotid endarterectomy was a common vascular surgical procedure and he would be back at his easel within a day or two.”
A lot has changed since everyman had his CEA in 1999. My practice in the 90s was to strongly consider referring my patients with asymptomatic carotid obstructions >70% for CEA, but as medical treatments for atherosclerosis advanced, since 2010 studies began showing minimal benefit in reducing stroke for CEA.
In 2022, I am rarely sent a patient who has not had a stroke or transient ischemic attack for CEA.
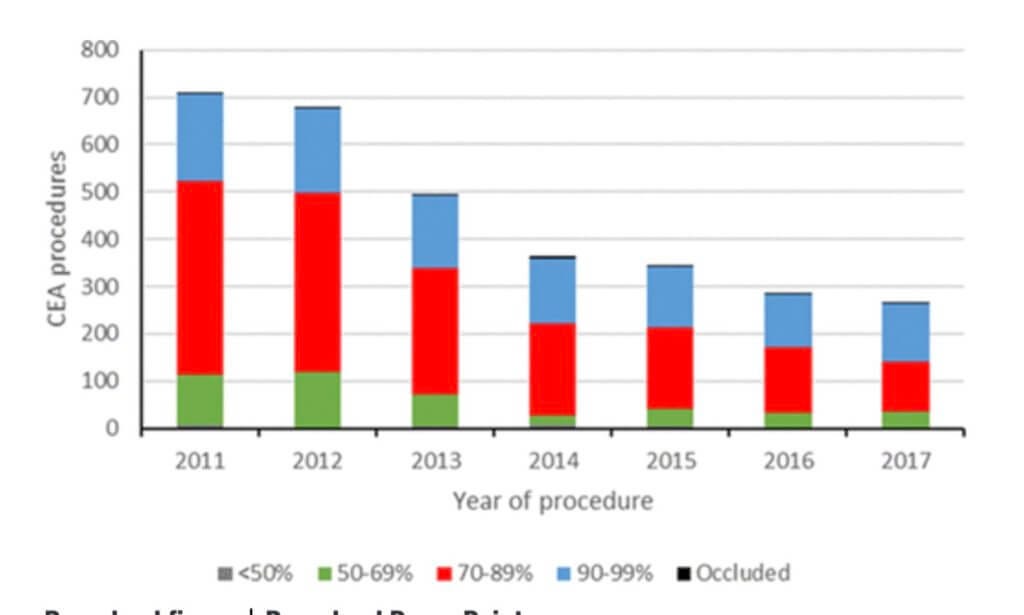
A recent British paper noted, “the role of CEA in asymptomatic patients has been a source of considerable controversy, with some countries performing large numbers of CEA procedures in asymptomatic patients (eg, the United States and Italy), while no CEAs are performed in asymptomatic patients in Denmark. Moreover, the latest Stroke Guidelines now advise against performing CEA in asymptomatic patients in Australia.”
This paper noted a 63% reduction in CEA performed in England on asymptomatic patients between 2011 and 2017.
The Choosing Wisely Project aims to identify low-value procedures and CEA in asymptomatic individuals with carotid stenosis >50% was in the top 5 for Australian/New Zealand Choosing Wisely Neurology Procedures:
"Don’t routinely recommend surgery for a narrowed carotid artery (>50% stenosis) that has not caused symptoms."
Best medical therapy is generally the appropriate management of patients with asymptomatic carotid stenosis. Medical treatment has improved since trials comparing carotid endarterectomy (CEA) plus best medical treatment with best medical treatment in asymptomatic carotid stenosis were conducted. There is evidence that the annual stroke rate in patients with asymptomatic carotid stenosis receiving best medical treatment has fallen to ≤1% annually. The effectiveness of CEA compared with current best medical therapy is not established. Additionally, randomised trials suggested equivocal benefit in women and patients aged >75. It may be reasonable to consider CEA for highly selected patient aged <75 years with >70% stenosis of the internal carotid artery. Where the perioperative risk of stroke, death and myocardial infarction is <3% and the patient is estimated to have a life expectancy of more than 3 to 5 years, consultation with a physician with expertise in stroke care is recommended prior to surgery.
Everyman is asymptomatic. He has had no symptoms from the obstruction in his carotid artery. There is no mention of stroke symptoms in the book and it must be assumed that Everyman, like thousands of Americans, is getting an unwarranted routine annual carotid ultrasound, the noninvasive test which allows the identification of asymptomatic plaque build-up.
It is important to note that many guidelines mention that CEA only makes sense in the asymptomatic patient if the preoperative risks of stroke, death and MI are less than 3%.
For a patient or referring physician to make an informed decision, therefore, they would need to know the surgical outcomes for the surgeon doing the procedure. In the real world, almost no one has this data.
The reason surgery for carotid blockages seems less helpful over the last 2 decades is similar to the reason that coronary artery stenting and bypass surgery is less helpful: improved medical control of atherosclerosis with lipid-lowering therapy, blood pressure control, and lifestyle changes including cigarette smoking cessation.
Unfortunately, we have no idea what medical therapy Everyman was getting. Given that statins were in widespread use by the mid-90s and given his history of coronary bypass surgery, he should have been on the most potent one available.
More Unnecessary Coronary Procedures
The year after his carotid artery surgery, Everyman "had an angiogram in which the doctor discovered that he'd had a silent heart attack on the posterior wall because of an obstructed graft." Given that Everyman mentions no symptoms related to this and given the previous inappropriately aggressive test and procedure ordering of his doctors, I can only presume that this repeat invasive angiogram was done because of an abnormal stress test.
Cardiology guidelines now recommend against the routine performance of stress tests following stenting or bypass procedures which I have discussed in detail here. This practice was the norm 20 years ago and persists to this day. A major concern with these routine tests is downstream testing like invasive angiograms which follow false positive results.
When inappropriate invasive angiograms are performed, coronary blockages are often found and stents are frequently placed that don't reduce the risk of heart attack or help symptoms. Sure enough, Everyman has a stent implanted in his LAD coronary artery, one which was not involved with the posterior wall of the heart at all.
The next year he gets another coronary stent, this time in a bypass graft. A year later he gets 3 more coronary stents. Again, no symptoms mentioned, no benefit obtained, other than to the pocketbook of the stenting doctor.
A Final Carotid Ultrasound Followed by Lethal Carotid Surgery
As we reach page 156 of this 182-page novella, Roth writes "When he next went to the hospital for the annual checkup on his carotids, the sonogram revealed that the second carotid was now seriously obstructed and required surgery."
As suspected, one of Everyman's doctors has been ordering a routine annual carotid ultrasound. Often, significant asymptomatic carotid stenosis is identified in screening studies prior to CABG. There are no good randomized trials to guide management of such cases. Some carotid stenoses are operated on simultaneously with the CABG, some sequentially and in lesser degrees, like Everyman's are managed medically.
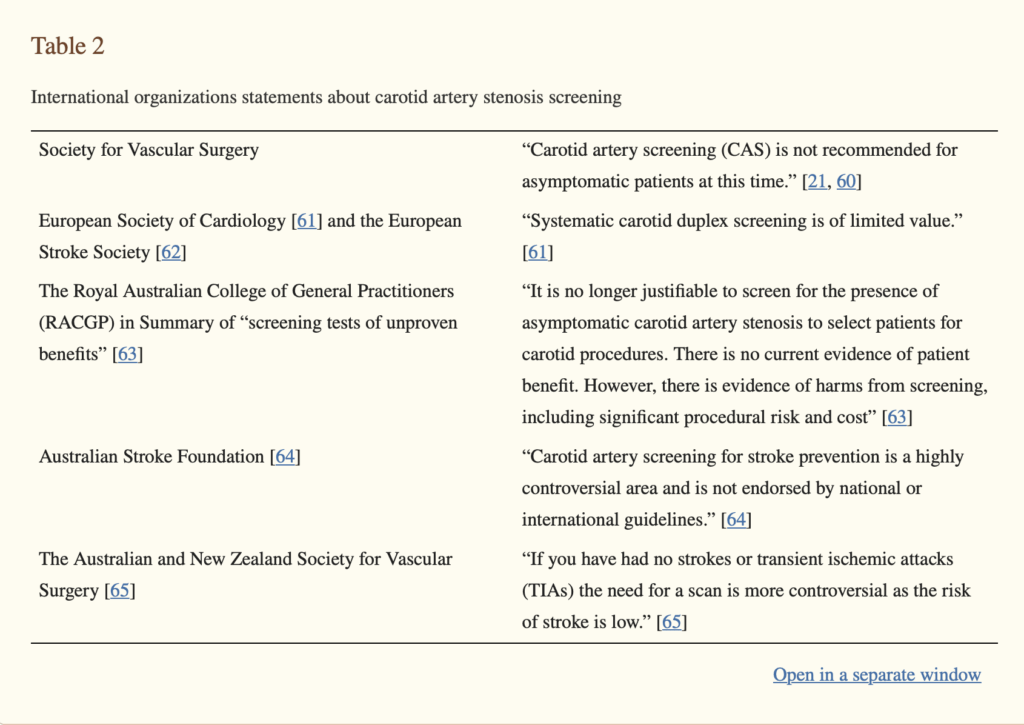
Outside the US, international organizations are pretty unanimous in condemning the routine screening of asymptomatic patients with carotid ultrasound
So, yes, Everyman was caught in the cycle of repetitive low-value annual carotid screening and it finally caught up with him.
Everyman requests general anesthesia "so as to make the surgery easier to bear than it had been under local anesthesia with the first operation."
Roth writes "He went under feeling far from felled, anything but doomed, eager yet again to be fulfilled, but nonetheless, he never woke up. Cardiac arrest. He was no more, free from being, entering into nowhere without even knowing it. Just as he'd feared from the start."
The fate of Everyman is not unique. How can today's patients avoid or minimize this carousel of cardiovascular testing, invasive procedures and potentially lethal operations?
Lesson For Patients
Decline low-value screenings like annual routine ECGs or screening carotid ultrasounds.
Strongly consider obtaining a second opinion when an invasive vascular procedure or major operation is recommended to you, especially if you are free of symptoms.
Ask your doctor why he is ordering imaging tests. How will the results change his treatment?
Remember that just because it seems logical to mechanically remove localized blockages in the arteries to our head or brain, the process of atherosclerosis which caused those blockages is diffuse and the optimal approach is most often a systemic medical one (see "Is coronary atherosclerosis a pimple versus a plumbing problem?")
Skeptically Yours,
-ACP
N.B. Roth indirectly suggests the choice of general anesthesia was a contributor to the death of Everyman, but a Cochrane analysis of 16 RCTS from 2021 concluded "The incidence of stroke and death were not convincingly different between local and general anesthesia for people undergoing carotid endarterectomy. The current evidence supports the choice of either approach. Further high-quality studies are still needed as the evidence is of limited reliability."